
In spite of my resolutions to write and podcast on something that more resembles an actual schedule, I have done neither recently. But my plea to the dozen of you that read this blog is to be forgiving: last week I had in-patient nose surgery to correct a deviated septum. In my case it was less deviated and more full-on deviant. Often, the septum can be corrected by septal resection: simply removing a portion of the cartilage and calling it a day; but my deviation was so extensive that doing this alone would cause my nose to collapse, and while that might be hilarious at first, it’s medically inadvisable; so my surgery was a septoplasty1, which is like a rhinoplasty, but less sexy, in that the nose gets shored up, either with bits of the patient’s cartilage or with a donor’s2.
I’m not over-sharing this out of a desire for sympathy while I convalesce (although flowers, chocolates, and bottles of scotch are welcome). Nor am I using solipsism as a crutch for not having other things to write about (not much, anyway). What I want to write about here is the way that, for all of the advancements in pharmaceuticals, imaging systems, and assistive robotics, surgery—and medicine in general—remains low-tech at heart.
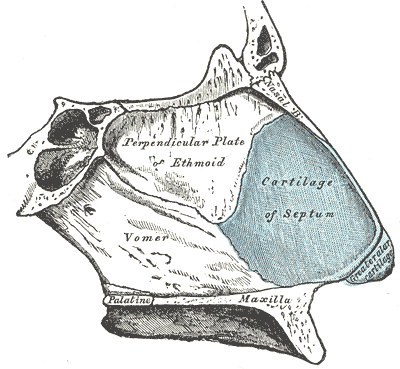
Reconstructing a septum has many similarities to carpentry: it’s a matter of cutting, positioning, and tacking. My surgeon had to use a hammer and chisel (or whatever they’re called in a surgical context) to pop my septum’s cartilage free from the bone. To allow my nostrils to heal in the proper open shape, I have had stents stuck in my sinuses like tiny cannoli tubes. Similarly, my post-surgery care has also been humble: flushing my nose with salt and water, and strapping a bit of gauze under the nostrils to soak up whatever falls out on its own due to gravity.
Back in the early 90s, when cable television kept adding odd networks in an attempt to convince viewers they were getting a bargain, there was a channel that consisted almost entirely of videos of surgical procedures, and since as I child I had wanted to be a surgeon, I watched these late at night3 with fascination. The one I remembered most vividly was a hip replacement in which the head of the femur was to be replaced with a polyethylene and steel prosthetic. The surgeons popped the bone free from its joint so that it stuck out like a rib in a rack of lamb, and then used a hacksaw to remove to worn-out part.
But the part of the procedure that was most memorable was when they hollowed the upper shaft of the femur so that the stem of the prosthetic could be inserted and cemented in place. One of the surgeons reamed out the femur using a long hand rasp, the kind you might have kicking around in a toolbox in the garage. I was shocked that such an imprecise tool, powered entirely by hand, was being used on a person. Recently I discussed this video with my son, who is his fourth year of med school, and he seemed unfazed, saying that it was about par for an orthopedic surgery, where so many involve mallets, saws, and screws.
Actually, I find it oddly comforting that at the end of the day we are made of physical stuff, and that there are people who have developed the skills to repair that stuff physically. It takes an enormous amount of knowledge, it takes substantial resources, and it takes procedures that have been developed painstakingly through generations. But it also takes a skilled, steady hand, patience, and pride of craft. It takes someone breaking things and sticking them together with stitches, screws, and glue. And I am lucky to have had the opportunity to get broken and fixed by a pro.
- Because nothing is ever easy, “Septoplasty” is sometimes used to refer to the removal of cartilage alone, or to the harvesting of said cartilage, or to the subsequent reconstruction, or to the whole enchilada of these procedures. And here I thought medical terms were all about precision. ↩︎
- In my case, my own cartilage was enough, so sadly I can’t now lay claim to a Frankenose. ↩︎
- I worked second shift. The joys of grad school! ↩︎
